IC and pelvic health
Bladder symptoms that won’t go away after a UTI.
Your urine culture cleared. The antibiotics are done. What lingers is pointing at something the infection test could not have caught.
By Intero · Updated June 15, 2026 · 8 min read
Intero is observational, not diagnostic. Journal content is informational only and is not medical advice.
Your UTI cleared but your bladder still feels off. Post-UTI bladder sensitivity, IC/BPS overlap, and why repeated antibiotic courses may not be the full answer.
A urinary tract infection has a clear path: symptoms, test, treatment, resolution. That is how it is supposed to work. For some people, it does. For others, treatment ends and something is still off. Urgency that lingers. Pressure that never fully went away. The feeling that the infection left something behind.
This experience is common enough to have a name: post-UTI bladder sensitivity. It does not mean the infection did not clear. It means the bladder may need longer to settle. Or that repeated infections have changed how the nerves around it respond to normal stimulation. In some cases, it points toward a condition that was already present, just masked by the UTI history.
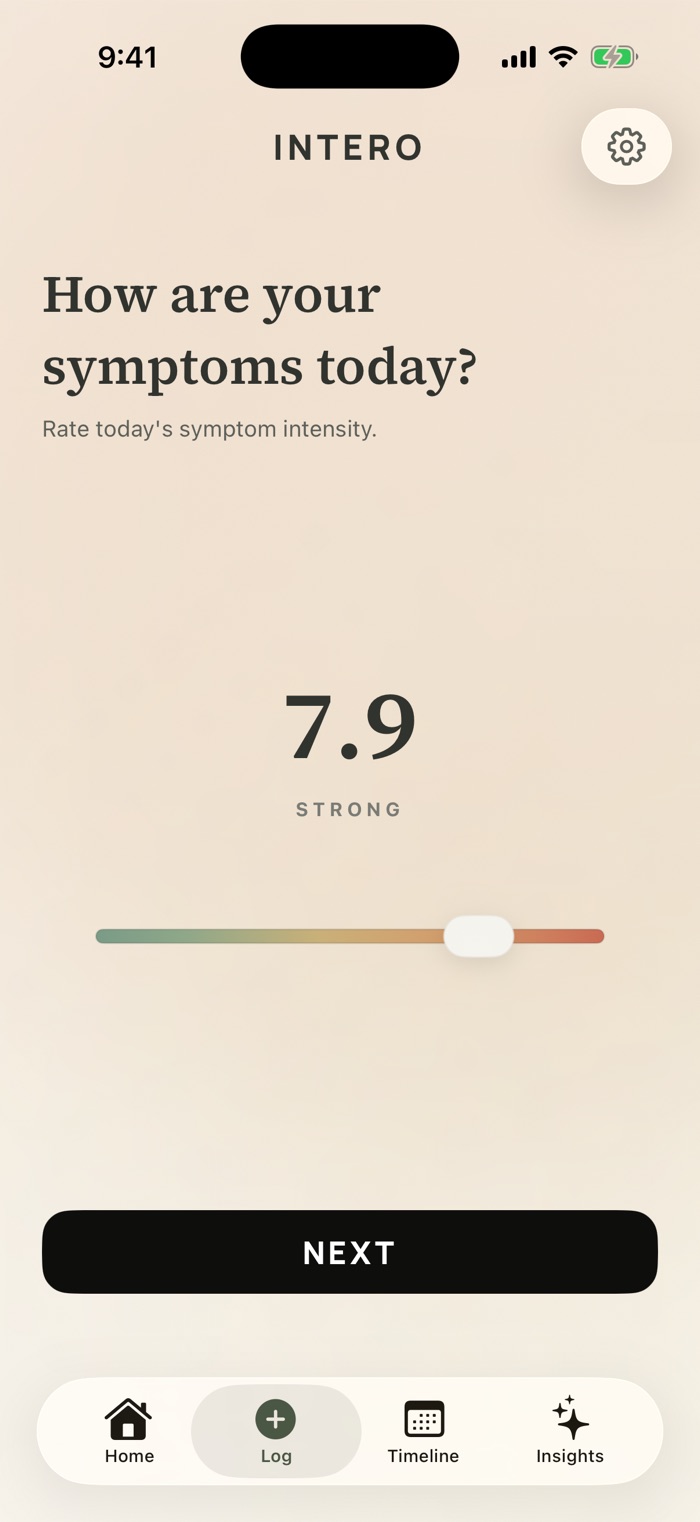
Download a printable symptom diary
Use the PDF today, or track the same symptoms on iPhone with Intero:
- Log urgency and frequency in seconds.
- See the pattern over weeks, not from memory.
- Bring a clearer symptom history to your appointment.
Why bladder symptoms can persist after an infection clears
A urinary tract infection is an acute event. The bladder tissue it affects is not. Repeated infection, or even a single severe one, can leave the bladder lining in a sensitized state. The bacteria are gone, but the nerve endings in and around the bladder have been through repeated cycles of inflammation. They do not always settle back down right away.
This is sometimes described as post-infectious hypersensitivity: the bladder responds to normal filling more intensely than it did before. The result is urgency, frequency, or discomfort that reads like an infection, even when no bacteria are present. The culture is clean. The symptoms are real.
How long this lasts varies. For some people, it resolves over weeks as the tissue calms down. For others, particularly after years of recurrent infections, the sensitization stops being temporary. It becomes the ordinary state instead.
Recurrent UTIs can mask a condition that has been there the whole time
Interstitial cystitis and bladder pain syndrome produce symptoms nearly identical to a urinary tract infection: urgency, burning, pelvic pressure, high frequency. The critical difference is that IC/BPS is not caused by bacteria. A urine culture will come back negative, or show only trace growth that does not meet diagnostic criteria.
For people who have had repeated UTI diagnoses and treatments, this creates a particular problem. If some of those episodes were actually IC flares rather than bacterial infections, the antibiotics would not have addressed them. But symptoms can fluctuate for other reasons. So the treatment looks like it worked, at least briefly. Over time, a pattern of "UTI treated, symptoms return" builds up without anyone looking beyond the cycle.
Among people with a history of recurrent UTI diagnoses, particularly those with consistently negative or low-count cultures, IC/BPS is more prevalent than the diagnosis rate reflects. The two conditions look identical in a single appointment. Antibiotics cannot treat something that is not bacterial in origin.
What the pattern looks like, and why it is worth writing down
There are specific features in a post-UTI symptom history that clinicians trained in bladder pain conditions look for. They include: cultures that come back negative while symptoms remain at full intensity; symptoms that return within days or weeks of completing a course of antibiotics; urgency or pressure that is present even when the bladder is not very full; symptoms that shift with stress, sleep, or certain foods rather than tracking with bacterial exposure.
None of these features alone confirms IC/BPS. But the pattern across time (how many episodes, how long symptoms lasted after treatment, whether there were stretches where things felt genuinely normal) is information a single appointment or culture cannot capture.
If you have been going through this cycle for months or years, the most useful thing you can bring to a urologist is a written record. Not a verbal summary, but specifics: how many episodes this year, what each culture showed, how long it took symptoms to return after each treatment, what your symptom-free stretches looked like. That kind of documentation changes what an appointment can accomplish.
When to ask for more than another antibiotic course
Most clinical guidelines recommend referral to a urologist after three or more episodes of bladder symptoms in twelve months, or if symptoms have persisted for more than six weeks after a completed antibiotic course. A urological workup goes further than a standard culture. It typically includes a closer look at bacterial counts, cystoscopy to assess the bladder lining directly, and a serious consideration of whether a bladder pain condition is driving what looked like repeated infection.
Pushing for this referral can be harder than it sounds. Recurrent bladder symptoms in women are frequently re-treated with antibiotics without investigation, even when the pattern suggests something else is happening. Having a documented history, written out with dates and culture results, makes that conversation more direct and harder to dismiss.
You are not asking a doctor to guess. You are showing them a pattern. That is different, and it gets different results.
Tracking what happens between infections matters as much as the infections themselves
One of the features that separates IC/BPS from recurrent UTI is what happens in the intervals, the stretches between episodes. In a purely bacterial recurrence pattern, symptom-free intervals tend to be complete: after treatment, things feel genuinely normal until the next infection. In IC/BPS, the picture is more continuous. There may be quiet stretches, but a low baseline of urgency or pressure persists. Flares arrive without a new infection. Certain days are harder than others for no obvious reason.
What symptoms looked like on ordinary days, not just the worst ones, is information that does not come out in a urine culture. It requires a record built over time: urgency levels across weeks, frequency across different situations, what happened around stress or sleep changes or certain foods. Not because any one data point is diagnostic, but because the pattern across them is.
If you are in the middle of trying to figure out what is happening with your bladder, keeping a symptom log is one of the most direct things you can do before your next appointment. Not to self-diagnose, but to bring something specific into a system that otherwise relies on a brief conversation and a urine sample.
Why this matters
Bladder symptoms that persist or return after antibiotic treatment are not always a new infection. Repeated cycles of treatment without lasting resolution can point toward post-infectious bladder sensitization or an underlying condition like IC/BPS that antibiotics cannot address.
A documented symptom record gives a urologist something specific to work with. How many episodes this year, what each culture showed, what symptoms looked like between infections. That shifts the conversation from repeated treatment to actual investigation.
Common questions
- Why do bladder symptoms persist after a UTI is treated?
- After a urinary tract infection clears, the bladder lining and surrounding nerves can remain in a sensitized state, sometimes called post-infectious hypersensitivity. This can produce urgency, frequency, or discomfort even when bacteria are no longer present. The duration varies; for some people it resolves in weeks, for others it persists longer, particularly after a history of repeated infections.
- What does it mean if my UTI symptoms come back after antibiotics?
- Symptoms returning after antibiotic treatment has more than one explanation. It could be a new bacterial infection, incomplete resolution of the original infection, or, particularly if cultures come back negative, a bladder condition like interstitial cystitis that was not caused by bacteria in the first place. If this pattern has repeated more than twice in the past year, a urological evaluation beyond a standard culture is generally recommended.
- Can recurrent UTIs cause long-term bladder problems?
- Repeated episodes of bladder infection can contribute to sensitization of the bladder lining and surrounding nerves, which may lower the threshold for urgency and discomfort over time. There is also meaningful overlap between recurrent UTI populations and people with undiagnosed interstitial cystitis, a chronic bladder pain condition that produces infection-like symptoms without bacterial involvement.
- How do I know if my bladder symptoms are IC and not a UTI?
- The clearest distinguishing feature is what a urine culture shows. A UTI is caused by bacteria and will show meaningful bacterial growth on a properly run culture. Interstitial cystitis produces nearly identical symptoms but without a bacterial cause: cultures come back negative or show only trace growth. If you have had repeated episodes with negative or inconclusive cultures, or if symptoms consistently return after antibiotic courses, that pattern is worth evaluating with a urologist familiar with bladder pain conditions.
Sources
- NIDDK: Urinary Tract Infections in Adults
- NIDDK: Symptoms & Causes of Interstitial Cystitis
- American Urological Association: Diagnosis and Treatment of Interstitial Cystitis/Bladder Pain Syndrome
- NCBI Bookshelf / StatPearls: Recurrent Urinary Tract Infections
- NCBI Bookshelf / StatPearls: Bladder Pain Syndrome